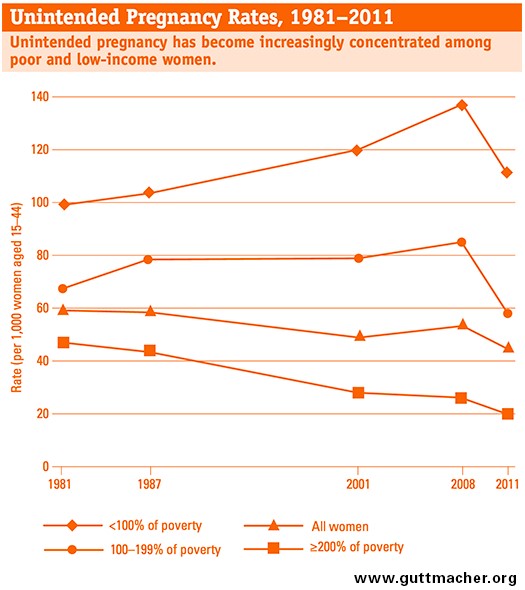
Last week, I pointed out that Planned Parenthood research spinoff Guttmacher Institute had removed a data-point from a graph on their website, which showed unintended pregnancies over the last 30 years for women in various income brackets. I criticized Guttmacher for this, and for stating that “After rising for most of the 30-year period beginning in 1981, unintended pregnancy rates among poor women have recently begun to decrease.”
This isn’t just statistical banter—this is important. By taking the data point out, Guttmacher furthers the Left’s narrative on abortion and birth control: that unintended pregnancies were constantly trending higher for poor women, and only when enough government began paying for intra-uterine devices (IUDs) from the likes of Planned Parenthood for America (PPFA) did this trend begin to slow.
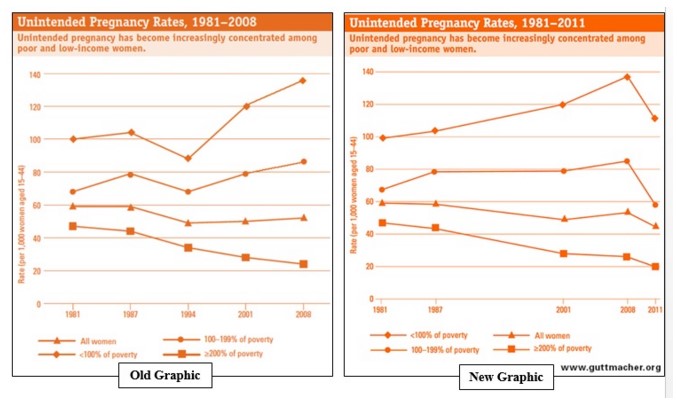
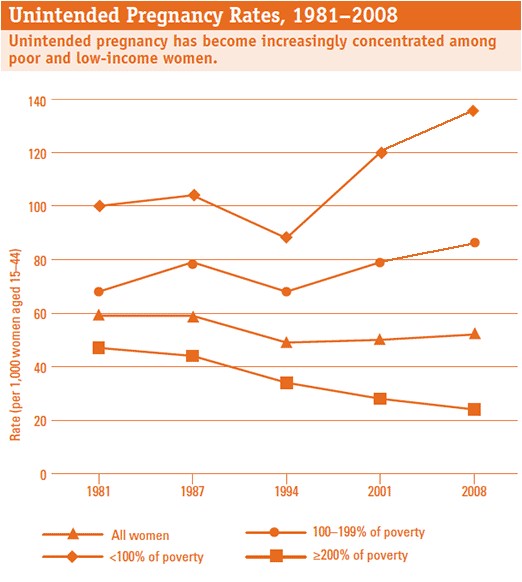
My main contention was that unintended pregnancy rates were falling for poor women before the mid-1990s (just as they were falling for women of all income-levels), but then spiked up in the late ’90s, even as unintended pregnancy rates continued to fall for well-off women. I said this divergence of outcomes for poor and rich women was due to a loss of contraception access among poor, mostly minority women in the mid-‘90s, just as Planned Parenthood got much larger and counted a greater portion of poor and minority women as customers. I have been using the chart, above and to the left, to say this since June of 2015.
Now, for the statistical banter. Joerg Dreweke, Guttmacher’s spokesman, took issue with my article in a series of tweets:
Dreweke is correct that Guttmacher’s reason for excluding the data-point was contained in a New England Journal of Medicine study (NEJM) corresponding to the information on Guttmacher’s website. I missed the study’s explanation for removing the 1994 data-point, and certainly should have noted it in my last article. That said, I had no intention to forgo Guttmacher’s side of the story, having given Guttmacher public relations employees nearly two weeks, full of repeated phone calls, to comment prior to the release of the article. They failed to do so.
The Data Still Supports My Conclusions
Dreweke is incorrect, however, to say that the central premise of the previous Federalist piece is false. First, Guttmacher shouldn’t have taken the data out. The NEJM study (released in March 2016, authored by Guttmacher) omitted the 1994 data point that fueled the original graph because “data on pregnancy intendedness were also collected in the 1995 survey of the National Survey of Family Growth (NSFG) but were excluded owing to concerns about the accuracy of the pregnancy intendedness data from that year.”
Guttmacher’s NEJM article then cites page 27 of an article several Centers for Disease Control statisticians authored in July 2012. In it, they worry that the 1995 NSFG survey overestimates intended births. So when Dreweke said the NSFG found problems with the data, he meant to say CDC statisticians had. The NSFG is a survey CDC conducts every six to seven years, which collects a range of data, including on the incidence of unintended births. While data is collected for the immediate period in which the NSFG is occurring, each NSFG also collects data on years that prior NSFGs have already covered.
What did the CDC statisticians say about the 1995 NSFG that caused Guttmacher to remove the 1994 data-point? It seems what most concerned them was that survey’s wide divergence on the rate of intended births for the years 1983-1987, compared with the 1988 and 2002 NSFG surveys: “Note that the estimate of the percentage of births intended in 1983-1987 is 60% from the 1988 NSFG and 60% from the 2002 NSFG, but 70% from the 1995 NSFG.”
The CDC statisticians said the variation was likely due to a programming error in the survey, which caused “a smaller-than-expected percentage of respondents to receive one of the questions leading to the question that captures whether the pregnancy was unwanted. So it is possible that this difference resulted in a smaller percentage of pregnancies classified as unwanted, and a larger percentage intended, in 1995 compared with the other NSFGs.”
However, although the 1995 NSFG report varies widely from the 1988 and 2002 NSFG surveys regarding intended births occurring in 1983-1987, the 1995 NSFG survey is much closer to the data for intended births in 1993-1997 (the period in question), found in the 2002 and 2006-2010 NSFG surveys. The 1995 NSFG finds births occurring from 1993-1995 to be 67.9 percent intended, while the 2002 and 2006-2010 NSFGs find the intendedness for births occurring from 1993-1997 to be 65.6 percent and 62.4 percent, respectively.
The CDC statisticians point out the fact that the 1995 NSFG is more accurate for births occurring within five years of 1995: “The percentage of cases imputed on this recoded variable was 5% overall and 3% for pregnancies in the 5 years before the survey. This is a relatively high percentage compared with the other NSFGs and could contribute to small differences in the estimates. Therefore, it was decided to omit the 1995 data from further consideration in this report. The authors remain confident of the quality and usefulness of the 1995 data for all other purposes [emphasis mine].”
Poor Women’s Unintended Pregnancies Definitely Dropped
It’s also not like the 1995 NSFG is the only NSFG survey that contains outliers. Data from other NSFG surveys not occurring in 1995 varies widely also. For example, the 2002 NSFG survey reports the percent of intended births in 1988-1992 to be 62.5 percent, while the 2006-2010 NSFG reports intended births in 1988-1992 to be 56.1 percent. In other words, all NSFG surveys seem to experience greater inaccuracy when estimating the intendedness of births going back more than five years before the survey. Yet Guttmacher has begun to choose which surveys to use and which to ignore, which just happens to reinforce Planned Parenthood’s policy goals.
Next, the CDC statisticians are on to something when they didn’t throw out the 1995 NSFG data entirely. The NSFG places births in three categories: intended, mistimed, and unwanted. To get to total unintended births, the CDC adds mistimed births and unwanted births. Remember, the possible error only affected the number of births reported as unwanted, not the number reported as mistimed.
Between the 1988 and 1995 NSFGs, unwanted births dropped 2 percentage points, from 12.4 percent, to 10.2 percent, respectively. Mistimed births, unaffected by any error, dropped from 26.7 percent in 1988 to 20.5 percent in 1995. In other words, of the almost 9 percent decline in unintended births from 1988 to 1995, from 39.1 percent to 30.6 percent, only a relatively small part of that drop was subject to any survey error.
That said, because unwanted births disproportionately occurred to poor women, unmarried women, and black women, by failing to count some births that should have been classified as unwanted, the 1995 NSFG survey does cause the 1994 data-point on the Guttmacher chart to exaggerate the drop in unintended pregnancy rates for women below 100 percent of the federal poverty level (FPL). Yet from 1988 to 1995, the rate of unwanted births occurring to black women declined from 29 percent to 21 percent. Was all of this really due to a survey error? During this same period, mistimed births to black women also declined.
Guttmacher itself has used the data from the 1995 NSFG as recently as July 2015, in its previous report on unintended pregnancies in the United States, almost three years after the CDC paper had called into question the 1995 NSFG data. When Guttmacher uses the CDC data, it (I believe rightfully so) tweaks the CDC data to fix the NSFG’s habitual undercounting of unintended pregnancy that ends in abortion. Doing so makes Guttmacher’s estimate of the percent of pregnancies that are unintended higher than the CDC estimate.
Guttmacher then calculates the rate of unintended pregnancies per 1,000 women, aged 15-44 years, based off of the number of unintended births that was estimated to occur in a given year. That’s how we get Guttmacher’s chart, and the disputed data-point on unintended birth rates for women below 100 percent of the federal poverty level in 1994.
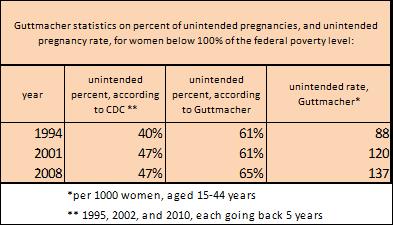
Note that the percent of pregnancies that were unintended, according to Guttmacher, didn’t change from 1994 (61 percent) to 2001 (61 percent). But the unintended pregnancy rate still increased dramatically, from 88 per 1000 women, to 120 per 1,000 women below the FPL. This increase in the unintended birth rate was largely due to more pregnancies among poor women, of which a constant portion were unintended.
In other words, because Guttmacher’s chart factors in abortions and overall pregnancy rates, even if the 1995 NSFG data from the CDC slightly overcounts intendedness, Guttmacher’s chart would still show a drop in the unintended rate among poor women in 1994, and a subsequent large increase in 2001.
In another example of this, the CDC’s percent unintended for poor women stays constant from 2001 to 2008, while Guttmacher’s rises from 61 percent to 65 percent, and its unintended rate for poor women climbs even higher to 137 out of 1000, mostly due to increased abortions among poor women during this period (in 2000, 26.6 percent of women obtaining abortions were below the federal poverty level, in 2008 42.4 percent of women obtaining abortions were below the FPL).
The Data Matches Facts on the Ground
Finally, the 1995 NSFG data showing a large drop in unintended births for poor and minority women doesn’t occur in a bubble of statistical hogwash. During this time, the managed care revolution was increasing Medicaid’s reimbursement rates to healthcare providers, which meant marginally greater access to primary care for poor women. Is it that hard to believe that greater choice led to better outcomes? Even Guttmacher’s lead researcher seems to attribute the drop during this period to increased birth-control pill use, not statistical error.
This is the same competition Planned Parenthood was lamenting in 1994, worrying that affiliates were on the verge of bankruptcy, because poor women receiving Medicaid were voting against Planned Parenthood with their feet, for providers that could offer a whole range of services over a provider that has a financial incentive to only care about abortion. In a business sense, Planned Parenthood is a dinosaur in the twenty-first century. No patient with buying power willingly frequents a provider with the small range of services found at a PPFA clinic.
What changed between 1994 and 2001? Planned Parenthood underwent an organizational shakeup, which included pushing out a CEO who wanted to combat the managed care revolution by turning clinics into primary care providers (given PPFA’s dinosaur status, this wasn’t going over well). Instead of competing with primary providers, PPFA chose to double down on its niche of being the family-planning provider to poor women.
PPFA lobbied for increased subsidization from the Clinton administration, and was helped by Planned Parenthood v. Casey, which drove out other providers competing to provide contraception to poor urban women, who were less national and less subsidized. All this allowed Planned Parenthood to grow substantially, tripling its overall revenues and abortion market-share between 1995 and today.
We Have Reason to Doubt the Left’s Narrative
In the end, Guttmacher’s removal of the data-point for the unintended birth rate among poor women in 1994 re-writes history far more than does leaving the data in. What’s the difference? The difference is the narrative. Are things just getting better now, or were they better before? After all the money PPFA spent on contraception for the poor, the PPFA/Guttmacher agenda says the money is finally working. If we want to keep it working, they need more funding.
This isn’t about a dot plot. It is about what the absence of that dot plot allows Guttmacher to say, and how this furthers the Left’s narrative on abortion and birth control: “Conservatives, Christians, Catholics, Evangelicals, Republicans… are all a bunch of hayseeds and religious nuts. We are pro-abortion, rabidly so, but because we want to increase funding for PPFA and the IUD, we will reduce abortions. PPFA does such great work. Conservatives are crazy for wanting to take away their subsidies. Don’t these hayseeds realize that taking away PPFA’s subsidies will mean more abortions? Subsidies should go up, not down!”
In its recent report on unintended pregnancies, Guttmacher says the unintended pregnancy rate for poor women is finally in decline: “After rising for most of the 30-year period beginning in 1981, unintended pregnancy rates among poor women have recently begun to decrease.” In other words, IUDs and PPFA began to turn the tide of a trend. Your average mainstream media journalist buys this narrative hook, line, and sinker.
From CNN: “A big part of the reason for the decline, at least so far, is the ‘pretty significant increase in women using long-acting contraceptive methods like the (intrauterine device) in recent periods’ [quoting Guttmacher’s lead researcher, Lawrence Finer].”
From NBC: “‘The clear implication for policymakers who wish to see fewer abortions occur is to focus on making contraceptive care more available by increasing funding and stopping attacks on all family planning providers.’ [quoting Dreweke]…Federal health officials and medical groups such as the American College of Obstetricians and Gynecologists say U.S. women need better access to birth control and to medical care so they know how to use it.”
From Vox: “LARCs (long acting reversible contraceptives) like IUDs and implants are amazingly, fantastically good at preventing pregnancy — better than any other available birth control. The fact that usage of these contraceptives has nearly tripled since 2007 (at least partially due to the Affordable Care Act) is a huge part of why unintended pregnancies are dropping.”
The Data Just Doesn’t Support Planned Parenthood’s Agenda
But the Left’s narrative is a lie. First off, state Medicaid already subsidizes the IUD and other LARCs, and PPFA still doesn’t give many out. In general, the Left’s obsession with IUDs is a bit weird, since most American women who use a LARC use the implant, not the IUD (also, the IUD is an abortifacient, while the implant is not).
Most important, saying that the unintended pregnancy rate among poor women is finally dropping due to IUDs, and funding for PPFA, is totally inaccurate. Even if the data from the 1995 NSFG is not as good as other available data, unintended pregnancy rates were, using what we know from other NSFG surveys, flat during that period.
The accurate telling of history is that between the late 1980s and 1994, the unintended pregnancy rate among poor women was going down, or was at worse unchanged. Even if it didn’t go down from 1987 to 1994, it was lower than it is today. This occurred in a time when IUD use was limited, and PPFA received less taxpayer funding. Then, suddenly, there was a big jump from 1994 to 2001, just as PPFA got bigger.
The media stories should be “unintended pregnancy rates for poor women finally dropping to where they were in the ‘90s, before things got really bad in 2001,” and “more competition needed among providers of healthcare for poor women,” not “unintended pregnancies are finally dropping because our liberal policies are working.”
This isn’t to say that IUDs don’t work, or that contraceptives are bad, or anything like that. It is to say that after all this money has been thrown at PPFA, to the extent that government has limited the choice of other contraception providers by granting PPFA a monopoly over taxpayer money for poor women, all this money has achieved worse outcomes.
Outcomes were better for poor women when PPFA’s Title X grant was much smaller, and when it served fewer customers. Does correlation mean causation? No. But we see what the lack of competition does with the Veterans Affairs, with your local Department of Motor Vehicles, and even with Comcast. Why not the same for PPFA?
Pro-lifers and conservatives should call into question the entire narrative from the Left with their own narrative. It sounds like this.
Progressives came along and broke up the poor family with the “Great Society” and fuel the sexual revolution. The fatherless children that resulted from this family breakdown created the political onus for abortion-on-demand, which culminated in the Roe v. Wade decision in 1973. Since then, progressives have been dumping taxpayer dollars on Planned Parenthood, with the hope that increased birth control funding will dampen the ill effects of their Great Society programs by reducing the poor’s rate of reproduction.
In doing so, progressives have created a special interest that receives taxpayer dollars, and in turn donates to and supports Democrats, the progressive party of the day. This special interest talks up birth control for poor women, but because it receives much higher profit margins for abortion, and presides over a captive market, this special interest has incentives that don’t align with the poor women it claims to serve.
Time for some trust-busting. Create a “women’s choice card” that allows women below 100 percent of the federal poverty level access to any OB-GYN in the country, for any service aside from abortion. If progressives’ special interest—PPFA—is so great, let it compete for this money, or let it go the way of the other dinosaurs.
Clarification: An earlier version of this article identified Guttmacher as a “research arm” of Planned Parenthood. Guttmacher and Planned Parenthood are no longer formally affiliated.