Back in 1987, Dr. Valenstein reminded attendees at a science conference to remember the history of the lobotomy. He warned that “all the major factors that shaped its development are still with us today.”
…desperate patients and their families still are willing to risk unproven therapies when nothing else helps. Ambitious doctors can persuade some of the media to report untested cures with anecdotal ‘research.’.…It could happen again.
I believe it is happening again—not with lobotomies, but pediatric medical transition. The treatment of “transgender” children is gaining significant momentum, despite the lack of research and regardless of the significant risks involved.
We can learn a lot by looking back at history. Here I revisit the rise and fall of the lobotomy and compare it to today’s enthusiasm for altering children’s bodies to match their gender identities.
A Short History of the Lobotomy in the United States
In the United States, the lobotomy pioneer and leading practitioner was Dr. Walter Freeman, a neurologist based in Washington DC. His story is featured in the hour-long 2008 PBS documentary, “The Lobotomist,” which I will quote throughout this article. Here is the full transcript.

In the spring 1936, Freeman came across a study conducted by Egas Moniz, a Portuguese neurologist, who took small corings from the brains of 20 patients with anxiety, depression, and schizophrenia. Moniz claimed the procedure eliminated symptoms in a third of them.
Freeman built on Moniz’s work. He thought disrupting the connections in the brain’s frontal lobes would bring patients relief from intense mental anguish. Freeman didn’t have a license to perform surgery, so he hired neurosurgeon James Watts.
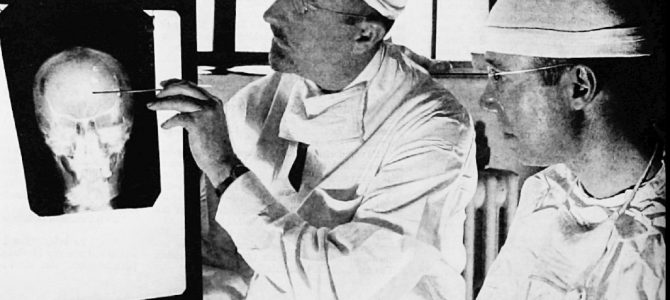
Later in 1936, under Freeman’s direction Watts performed their first lobotomy. He made incisions on the patient’s head, drilled holes through her skull, inserted a small spatula-like instrument into her brain, and sliced through neural fibers connecting the frontal lobes to the thalamus. Four hours later, she woke up alert, but calm.
They felt emboldened to perform more Freeman-Watts standard prefrontal lobotomies. After just a dozen, they were ready to declare the procedure a success even though some patients relapsed (which prompted second, and sometimes third, operations), and even if post-op patients had reduced intelligence, were unmotivated and lacked emotional depth.
Eventually Freeman sought an easier, quicker way to lobotomize patients. By 1946 he had devised a new method to access the brain using simple tools—an ice pick and hammer. (The first ice pick was actually taken from Freeman’s kitchen drawer. But modifications were made over time. The tip on earlier versions occasionally broke during the procedure.)
“Freeman would peel back each eyelid, insert his ice pick and with a hammer tap through the brain, wiggle it about, sever the frontal lobes, withdraw it,” Andrew Scull, a sociology professor, told PBS. “And when the patient came to, he or she would be given dark glasses to hide the black eyes they’d been given.”
Freeman did the transorbital lobotomies himself, sometimes in his office. It took only a matter of minutes. He did not require an operating room and the equipment was portable, which made it convenient for travelling to mental asylums. At this point Watts, who had grave concerns about those without formal surgical training performing the “ice pick” lobotomy, ended their partnership.
The Press Raves at a ‘Miracle Cure’
Initially the procedure was heralded in the press as a miracle cure. Many sought out lobotomies for themselves or their loved ones. Enthusiasm flourished until the mid-1950s when an antipsychotic drug called Thorazine, promoted as a “chemical lobotomy,” became increasingly used. Around this time, the poor outcomes from the first clinical trials were also published. The procedure fell out of favor and was recognized as barbaric and Freeman a charlatan.
Freeman moved to California, but didn’t give up on lobotomies. He cultivated new categories of patients to treat. Disaffected housewives, people with chronic headaches, and misbehaved children were all fair game. Nineteen of Freeman’s patients were children under the age of 18. One was only four years old!
Freeman continued performing lobotomies until 1967. He may have kept operating if his hospital privileges had not been revoked. The hospital took this action only after one of Freeman’s patients died from a brain hemorrhage following her third lobotomy.
The history of this medical fad reveals that pioneering doctors, and the medical establishment that embraces them, can fail in their duty to “Do No Harm.” It shows people, even those who possess medical degrees, are imperfect and can champion poor science.
At initial glance, it may appear that lobotomies (which target assumed defects of the brain) and the medical transition of gender dysphoric children (which target assumed defects of the body) have little in common. But if you look past which body parts are “corrected,” you see that both are psychological conditions some doctors treat with drastic, irreversible medical interventions. There are a number of parallels.
1. A High Level of Desperation
Both lobotomies and now the medical transitioning of young people have been more easily accepted because of their environment. A sense of hopelessness paired with yearning for a cure leads people to take chances they wouldn’t normally.
In the 1930s, there were no anti-psychotic drugs to ease patients’ intense suffering. Freemen justified lobotomizing the mentally ill due to their high suicide rates. He felt that a “surgically induced childhood” was beneficial and outweighed any potential risks.
During this time, people suffering from severe mental illness were warehoused in overcrowded, underfunded mental asylums. The conditions were horrible. Some were tied up on benches. Others lay naked on the floor. Feces were sometimes smeared on the walls. Conditions became further strained with the return of shell-shocked World War II veterans.
There was a huge impetus to find treatments to alleviate sufferers’ symptoms and allow them to go home to their families. When lobotomies were introduced and touted as a cure, many chose to have loved ones undergo the procedure, rather than admit them to one of these notorious institutions, like the one exposed in this newspaper story:

Currently, whenever the media discusses a transgender-identifying child, without fail they mention a high suicide attempt rate. Gender specialists imply that children will die unless fully “supported” in their chosen gender identities. We are told that proper pronouns, new clothes, a chest binder, puberty blockers, cross-sex hormones, and surgeries may be necessary just to keep them alive.
This is just one of many examples found in today’s media coverage of trans-identifying children: “Neal found a therapist who told her and her husband to fully embrace Trinity’s female identity. She said that the therapist also gave strikingly blunt advice. ‘She said, ‘Your daughter already knows who she is. Now you have to decide. Do you want a happy little girl or a dead little boy?’”
Gender specialists and trans activists continually scare parents with high suicide attempt statistics from a flawed survey that did not ask whether suicide attempts occurred before or after transition. Neither did it control for co-occurring mental health problems. Actually, one long-term study has shown that suicide rates are significantly higher in those who have medically transitioned compared to those of the general population.
Many highly publicized suicides of trans-identifying teens were young people who had been fully supported in their transitions Additionally, gender-affirmative care has become enmeshed in the transgender rights movement. Well-funded civil rights organizations (including, but not limited to, the American Civil Liberties Union, the Human Rights Campaign, and the NCLR) campaign for children to be affirmed in their gender identities and given access to medical interventions that will transform them into their “authentic” selves. Organizations like Gender Spectrum and Gender Diversity are in schools training staff and students in transgender ideology. Democrats have made transgender rights a part of their platform.
2. Someone Besides the Patient Authorizes Treatment
During the lobotomy craze, many patients were not able to consent to the procedure themselves. Parents, spouses, and siblings were called upon. Many opted to have their loved ones lobotomized based upon a professional’s recommendation. Often they were given false hope and not informed of the serious side effects. Due to press’s lavishing praise, some people actually demanded their relative receive a lobotomy.
Currently, parents are responsible for approving medical interventions for their under 18-year-old gender dysphoric children (although in Oregon it’s possible for 15-year-olds to get double mastectomies or other surgeries without parental consent). Based on media coverage, it appears that quite a few parents are approving treatment.
A parent’s choice of what direction to take is highly influenced by the information they rely upon. Many gender specialists and the media paint a pretty rosy picture of what life can be like for children if they are affirmed in their gender identity and given body-altering treatments so they can pass as the opposite sex. But this is an optimistic belief, based on opinion and anecdote, not solid evidence.
3. Highly Variable Results
Lobotomy outcomes were all over the map, which isn’t surprising if you consider the procedure was an imprecise “stab in the dark.” Freeman’s patients—ranging from severely mentally ill adults to misbehaving children—also had a wide variety of symptoms pre-treatment. Lobotomy outcomes generally could be divided into three categories: “Drs. Freeman and Watts considered about one-third of their operations successes in which the patient was able to lead a ‘productive life’…Another third were able to return home but not support themselves. The final third were ‘failures,’ according to Dr. Watts.”
Although they were relatively rare, some patients were fortunate enough to have no noticeable side effects. For them, having a lobotomy appeared to bring great relief. But the majority of patients with successful outcomes still had concerning side effects. They often became childlike, lost their ambition and weren’t able to make judgments or function well socially. Most were significantly changed, never to be the same person again.
Here are some before and after lobotomy pictures (Case 121, 1942). Before: “Forever fighting…the meanest woman.” After: “She giggles a lot.”
A significant number of post-op patients were reduced to a persistent vegetative state. And for others, the operation was fatal. The PBS narrator says “At Cherokee state hospital in Iowa, three of Freeman’s patients died on the operating table, one after Freeman’s ice pick slipped while he was taking a photograph. Without pausing, he packed up and left for his next demonstration.”
Statistics from the Veterans Administration (which performed approximately 2,000 lobotomies), kept track of how many died as a result of the procedure: “The VA did try to determine whether the benefits outweighed the risks. And the risks were severe. Overall, 8% of lobotomized veterans died soon after the operation, according to a 1947 document. One hospital reported a 15% fatality rate.”
There are a variety of outcomes from medical gender transitions as well. Some people say transitioning is life saving. Some react poorly to cross-sex hormones or have surgical complications. Some decide to de-transition or re-identify as their natal sex. Some even die due to medical transition itself (here is an analysis of a 2014 Dutch survey study in which one patient died from complications of surgery).
4.Treatment Based on Theories, Not Solid Evidence
As Freeman and Watts’ patient caseload grew, they gained confidence in their technique and wanted to share it with colleagues. They presented their findings at a Baltimore medical conference and declared they’d found a cure for mental illness.
Some in the audience vociferously opposed Freeman and Watts. They were shocked that anyone would consider surgically damaging brains a good idea. They were astonished by the lack of research. Since it was not considered ethical to publically criticize a fellow physician, opposing viewpoints were muffled. Freeman was undeterred and plowed ahead.
There is a lack of research that backs up the medical transition of children. The current protocol being used in the United States is based on best guesses, not solid evidence. The gender affirmative approach, which advocates “supporting” children in their chosen gender identities, is a theory that has not undergone rigorous study. Puberty blockers and cross-sex hormones are being used off-label, their side effects are unknown in still-growing bodies. Some teens have even undergone mastectomies, hysterectomies, and genital surgeries.
In the United States, the first pediatric gender clinic opened its doors in 2007. But it wasn’t until May of 2016, almost a decade later, that a National Institutes of Health-funded study recorded the effects of puberty blockers and cross-sex hormones on young people. The patients will be followed for five years. All of the unknowns, however, aren’t stopping practitioners.
5. The Power of the Press
Freeman used the media as a promotional tool. He often arranged for journalists and photographers to cover lobotomy demonstrations at mental asylums. “The Washington Star called lobotomy ‘One of the greatest surgical innovations of this generation.’ The New York Times called it ‘surgery of the soul,’ and declared it ‘history making,’” the PBS documentary says.
In 1941, the Saturday Evening Post described the transformation of a lobotomized patient: “A world that once seemed the abode of misery, cruelty and hate is now radiant with sunshine and kindness to them.”
A 1999 study analyzed popular press coverage of the lobotomy and its potential influence on how quickly acceptance of the procedure spread. The abstract says (emphasis added):
This study analyzed the content of popular press articles on lobotomy between the years 1935 and 1960. Both a qualitative and quantitative analysis provided evidence that the press initially used uncritical and sensational reporting styles, with the content of articles on lobotomy becoming increasingly negative through time. The initial positive bias occurred despite opposing views in the medical community, which provided a basis for more balanced coverage. These findings support the theory that biased reporting in popular press articles may have been a factor influencing the quick and widespread adoption of lobotomy as a psychiatric treatment.
I don’t know if you caught that, but journalists often omitted “opposing views in the medical community.” In 1941, the American Medical Association issued “a warning about several negative effects on personality including apathy, inappropriate social behavior, and lack of initiative (i.e., the frontal lobe syndrome).”
Also of interest in the study were these statements: “In addition to sensationalizing the positive effects of lobotomy, articles during this time period rarely discussed risks involved in the operation” and “…in most cases mention of negative side effects was either absent or cursory.”
Currently there are nearly daily examples of trans kid media stories. They tend to be pretty formulaic. From an early age, the child realizes he or she feels different from peers. A girl that throws a fit when mom puts her in a dress; a boy that wants to wear a dress. In general, preferences in clothes, toys, and haircuts are used to validate that they’re transgender.
The child (or parent) finds out about transgender through the Internet, radio, or television, and latches onto that explanation. They either want to avoid the “wrong puberty” or have struggled through puberty and want to correct their bodies with cross-sex hormones and surgeries.
Parents sometimes admit they didn’t immediately believe their child was transgender. But when they learn of the suicide statistics, then they get on board. To drive the point home, the article quotes a purported expert in the field who states unproven theories as if they were settled science.
With few exceptions, journalists focus on the feel-good aspect of the child being accepted as the opposite sex, a triumph over adversity. Not much time (if any) is spent discussing opposing views in the medical community or the significant risks associated with medical interventions. Biased media coverage like this is likely contributing to the rapid increase in children presenting to gender clinics.
6. An Embrace from Doctors
Initially many of Freeman’s fellow doctors were reluctant to embrace the lobotomy as an acceptable treatment, but that soon changed. Thanks to favorable newspaper articles, Freeman became somewhat of a celebrity. The public believed he had found a miracle cure. His services were sought.
Additionally, some state-funded mental asylums were so financially strapped that they were on the verge of closing. Freeman began travelling to these institutions, promoting lobotomies as a cost-cutting measure. The more patients discharged, the greater the savings; and the patients who remained were more manageable. Freeman even convinced the federal government via the Veterans Administration to perform lobotomies.
In 1948 Freeman was elected president of the American Board of Psychiatry and Neurology. In 1949 Moniz, whose work inspired Freeman’s procedure, was awarded a Nobel Prize for psychosurgery (Freeman had nominated him). The lobotomy gained further credibility. By 1950, elite medical facilities, including Johns Hopkins, Mass General Hospital, and the Mayo Clinic were performing lobotomies.
Currently, there appears to be widespread acceptance of medical interventions for gender dysphoric youth. Clinics all across the country provide gender care. It’s becoming more common to obtain insurance coverage for puberty blockers, cross-sex hormones, and surgeries. Some states have passed laws that forbid therapists from attempting to change children’s gender identities. Many mental health professionals seem to believe their duty is to simply affirm children’s beliefs, not to explore why they feel they’re the opposite sex.
A number of organizations, including the AMA and the APA, declare support for transgender people in health care.
7. Expanding the Patient Base
Freeman barnstormed mental asylums, operating on many patients in each location. He was frequently gloveless, mask-less and sometimes sleeveless. Once he performed 25 transorbital lobotomies in a single day.
He enjoyed shocking his audience. On some occasions, Freeman would start out operating using his right hand, and half way through switch to using his left hand. Other times he would an insert ice pick under each eyelid and simultaneously lobotomize through both eye sockets. Sometimes doctors in the audience would faint, or even vomit.
While at the institutions, he trained others in his craft. Freeman claimed that “Any damned fool, even a hospital psychiatrist, could learn it within an afternoon.” A zealous recruit in Texas racked up 75 lobotomies in one day. Thanks to Freeman’s mentoring and dogged salesmanship, lobotomies steeply increased—from 150 in 1945 to more than 5,000 in 1949.
For pediatric gender care, the actual patient numbers in the United States are difficult to determine. But based on the fast-paced expansion of gender clinics across the nation, the patient load has likely escalated similarly to what has been seen in the UK:
The first gender clinic in the United States opened in 2007 in Boston. An October 2016 article states there are now more than 60. Based on this information, in conjunction with the growing number of 4thWaveNow parents (many who note the number of trans-identifying students in their local schools are multiplying), it appears that the cases of young people with gender dysphoria are skyrocketing.
8. ‘Correcting’ Sexual Orientation
Up until 1973 homosexuality was considered a mental disorder. Lobotomies were sometimes performed to “correct” sexual orientation. The current practice is to treat prepubescent trans-identifying kids with gender affirmation and puberty blockers. But according to decades of research, 60 to 90 percent of gender dysphoric children, if left alone, grow out of their distress. Most mature into lesbian and gay adults.
Puberty is often the time gender dysphoria starts to resolve and sexual orientation begins to be self-recognized. Early interventions by gender specialists likely prevent many young people from ever becoming comfortable in their unaltered bodies. Furthermore, the vast majority (some clinics report 100 percent—see here and here) of children on puberty blockers proceed to cross-sex hormones, irreversible sterilization, and possibly later surgeries.
9. Earlier Interventions to Prevent ‘Problems’
Initially Freeman claimed the lobotomy would be an operation of last resort. He once said, ”I won’t touch them unless they are faced with disability or suicide.” But as time went on he started advocating for lobotomy earlier, as a way to prevent mental deterioration. In a 1952 Time article (“Mass Lobotomies”), he is quoted as saying, “it is safer to operate than to wait.”
The push for early intervention is also seen in medical transition of “trans” kids. Initially it was reserved for gender dysphoric adults, but now children are increasingly being treated. The justification: if gender dysphoria is caught while they are young, they can avoid the years of misery that many older trans people report.
It is assumed that treating children earlier will help them appear more convincingly as the opposite sex. This, along with consistent affirmation of their gender identity, is assumed to help these children avoid suicidality, depression, unemployment, sexually transmitted diseases, drug abuse, and homelessness commonly found in the current adult transgender population. Gender doctors state they are saving these children from potential future problems (without acknowledging the significant risks treatment introduces).
10. Ambitious Doctors
Freeman came from a prominent medical family. His grandfather, William Keen, was a famous surgeon, the first to extract a brain tumor from a living patient. Freeman looked up to his grandfather and wanted to be as successful. Early in his career Freeman became determined to alleviate patients’ emotional torment. He spent countless hours examining the brains of dead mental patients, trying to find a defect which could be corrected. But he was never able to find any.
He was thrilled to come across Egas Moniz’s work, and latched onto lobotomies as a way to bring patients a sense of peace. Freeman appeared to genuinely believe he was helping people by lobotomizing them, but seemed blind to the negative impacts of his procedures.
“One of the characteristics of an enthusiast, and Walter Freeman was certainly that, is that they are able to overlook everything that contradicts their enthusiasm. And they concentrate on all the things they see that show they’re on the right path. So over and over again, we can see Freeman managing to dismiss the casualties of his surgical interventions,” Scull told PBS.
In 2007, endocrinologist Dr. Norman Spack co-founded the first U.S. pediatric gender clinic in Boston. Spack frequently talks about suicide rates in media interviews, saying “almost one in three trans individuals will attempt suicide if they do not receive treatment until after puberty.” He is a big proponent of using GnRH-agonists to pause the puberty of gender-distressed children. Gender specialists often describe puberty blockers as “safe,” “reversible” and “life saving,” but many have reported severe side effects, especially when administered to children.
Spack says treating gender dysphoria is less complicated than it would seem: “You don’t need to be a rocket scientist to take care of a transgender patient.” In 2012, it was reported that Spack has trained many gender professionals across the United States and Canada. His program has spread to more than 60 pediatric gender clinics in the United States.
Many parents are concerned we may be in the midst of another disastrous medical fad. Our kids’ sudden change in gender identities has been easily accepted by their peers, schools, therapists, and doctors. Puberty blockers, cross-sex hormones and surgeries are routinely encouraged as necessary next steps. The level of enthusiasm is stunning. There’s an absence of caution. We don’t know how many young people will grow up to regret their permanently altered bodies.
The uncritical championing of child transition will eventually fizzle. Lessons will be learned. Science will evolve. Eventually books and documentaries may try to explain how things got so out of hand. How long that will take is anyone’s guess.
A version of this article first appeared on 4thWaveNow, a blog for LGB-supportive parents concerned about the increasing trend to medically “transition” gender-nonconforming youth.







{kind=link}