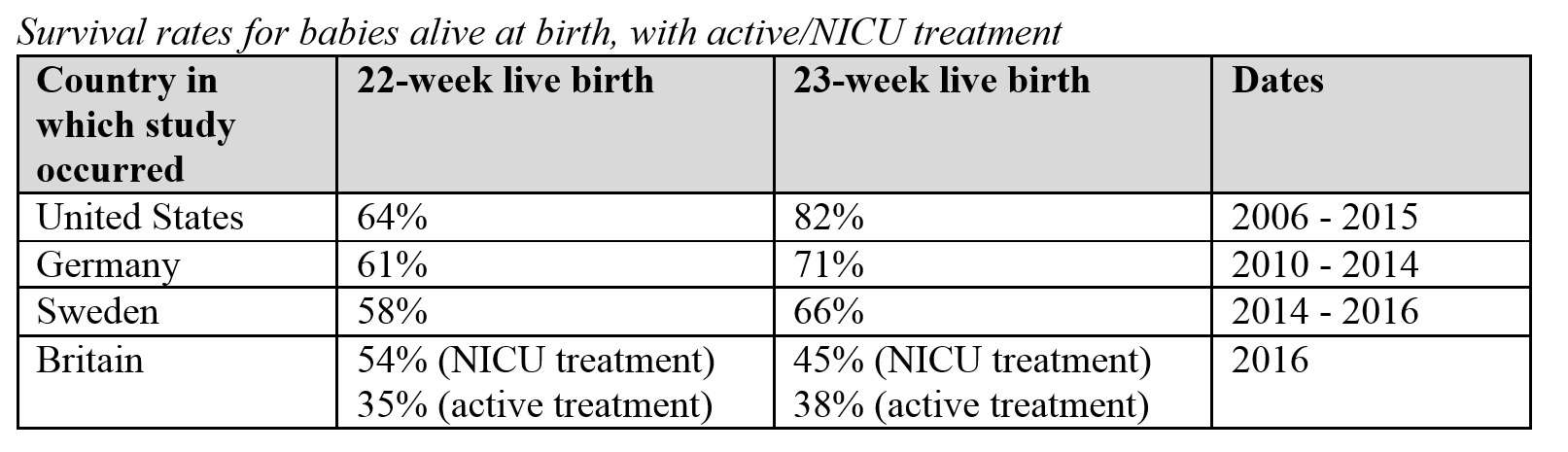
Statistics for the survival of premature newborns are increasingly optimistic. A study at the University of Iowa found that 64 percent of 22-week babies and 82 percent of 23-week babies who were alive upon delivery and whose parents wanted resuscitation survived to hospital discharge (one baby in the sample was excluded because of a congenital anomaly).
According to a study in Germany, 22-week babies who showed any sign of life after birth and who were given active treatment had a 61 percent survival rate, while 23-week babies had a 71 percent survival rate. Doctors did not determine whether to give active treatment based on infants’ characteristics but left the decision to parents. For infants given active care and those given only palliative care, there were no significant differences in birth weight or whether infants were singletons or part of multiples.
A study in Sweden found that 58 percent of 22-week infants and 66 percent of 23-week infants who were admitted to the NICU survived. After the British Association of Perinatal Medicine examined Britain’s encouraging survival rates (54 percent for 22-week infants and 45 percent for 23-week infants treated in the NICU) as well as those from the international community, it recommended in 2019 that clinicians consider treating 22-week infants if the babies show favorable characteristics.
See the table below for survival rates from these four studies. Additionally, the University of South Alabama Children’s and Women’s Hospital reports on its website that its survival rate for 22-week babies is just under 70 percent.
Despite all these findings, current medical guidance in the United States is to recommend resuscitation for babies born at 24 weeks and to only consider resuscitation for those born at 22 and 23 weeks.
There is wide variation in whether U.S. hospitals are willing to treat 22-week and 23-week babies. One study showed that most sampled hospitals did not treat 22-week infants, and some did not treat those born at 23 weeks. Parents tell heartbreaking stories in which they were unable to convince clinicians to treat their newborns, even at hospitals with Level 3 NICUs, the recommended facility for this age group.
A new standard of care could affect thousands of babies per year. There were almost 4,600 22-week and 23-week babies born alive in the United States in 2017 (1,829 and 2,767 babies, respectively). Extrapolating from the U.S. data in the table above, the right treatment could result in an estimated 1,170 22-week babies and 2,269 23-week babies surviving per year.
Often clinicians do not attempt to administer life-saving care to such preemies because the infant is at increased risk of disability as a result of the prematurity. However, parents should know that for an individual infant, it is impossible to know whether the child will have any disabilities because he is born early.
The British Association of Perinatal Medicine defines severe disability as an IQ lower than 55, severe cerebral palsy, blindness, or profound hearing impairment. It examined its data and concluded that a minority of the children (approximately one-third of 22-week babies and one-quarter of 23-week babies) had a severe disability.
The study from Germany reports that, of the 22- and 23-week infants for whom it had follow-up data, half showed at least some level of neurodevelopmental impairment at two years corrected age. It also found that 75 percent of the infants experienced severe complications, including intraventricular hemorrhage of grade 3 or 4 (bleeding in the brain) and bronchopulmonary dysplasia.
This presents a larger question of whether clinicians should treat patients with potentially chronic health issues that are burdensome or painful. If only the healthy are considered worth saving, then it would follow that because of these babies’ increased risk of disability, they should not be given active care. If human life is worth living even if it includes suffering and disability, then it would follow that clinicians should try to give these children their one opportunity at life.
However, every newborn’s situation is unique, and other complicating factors, such as an infant’s malformed organ system or a lack of adequate hospital equipment, make mandated resuscitation unwise. The risk-benefit ratio must always be considered. Care should not be overly burdensome to the infant with minimal chance of success.
Given: 1) the mounting optimistic data for survival rates; 2) the relatively large number of infants who could potentially survive each year; 3) the recognition that it is impossible to know at birth if the newborn will be disabled because of her prematurity; and 4) the idea that chronic health issues do not mean that a life should end, clinicians and hospitals should move towards a new standard of care.
Policymakers and clinicians should take action on the newest data, rather than relying on historical survival rates. These survival rates are abysmally low because treatment for these infants was mostly withheld.
Hospitals should train staff in a new standard of care for 22- and 23-week babies and use performance-improvement projects to measure and advance their progress. They should consult national and international experts to help them reach what is theoretically possible. Hospitals that do not have the ability to resuscitate these infants should have protocols to quickly transfer patients to equipped facilities and manage patient care before and during transfers (e.g., administration of antenatal corticosteroids and magnesium sulfate).
Additionally, clinicians should provide parents accurate data, helpful resources (e.g., support groups or adoption resources for parents who do not know if they can care for a child with disabilities), and unbiased counseling (e.g., avoiding claims without evidence, such as “no chance of survival”).
Further, hospitals should make their resuscitation policies easily accessible to the public. They should also be transparent regarding what gestational ages are routinely cared for in their NICUs and what is available at nearby hospitals’ NICUs.
Just like all hospitals do not have the capacity to offer all surgeries, not all NICUs are ready to care for a baby born at 22 or 23 weeks. Parents who are faced with imminent delivery for this age group should be able to quickly access information on whether the hospitals will treat their infants so they can make informed choices before deciding where to deliver.
An advocacy group called TwentyTwo Matters has assembled a map of hospitals that have saved at least one 22-week baby, as reported by parents who follow the group on social media. This is not an exhaustive list of hospitals. Also, with changing circumstances, hospitals on the list may no longer treat 22-week babies. The community-assembled, incomplete map highlights the need for hospitals to make resuscitation information publicly accessible.
TwentyTwo Matters advocates can help parents one on one who are facing an imminent delivery (parents can send them a message here). The group’s social media pages feature many encouraging stories of infants and children who were born at 22 (or 21) weeks as well as those of babies who were refused anything other than comfort care. The group is available on Facebook, Twitter, and Instagram.
The potential for an updated standard of care for infants born at 22 and 23 weeks shines a harsh light on U.S. abortion laws, which in some states extend to the full nine months. Every year in this country, there are more than 11,000 babies at 21 weeks gestation or later who are killed by abortion.
According to the pro-choice research organization the Guttmacher Institute, most elective abortions at 20 weeks or later are not because of any health issues with the child. A sizable proportion of those killed could survive if they were instead delivered and given the right treatment, which suggests a possible alternative option for these mothers. Additionally, recognizing the viability of 22- and 23-week infants will perhaps inspire a greater respect for those of the same age inside the womb.
The U.S. treatment protocol for 22- and 23-week newborns must be grounded in the latest science and in clinical judgment for each newborn’s unique circumstances. Policymakers, hospitals, and clinicians should take action now to improve their care.
Drs. Robin Pierucci and Donna Harrison both contributed to this article.