
As a group of suburban Portland psychiatric nurses sat for training in late 2016, they had no idea they were witnessing a paradigm shift in public health policy. They simply wanted to know what to do about a sudden upsurge in young psychiatric patients who believed themselves to be in the wrong body. They had turned to a colleague from Oregon Health and Science University (OHSU) for help.
The reply was astonishing: The children’s claims should be taken at face value, and the children should be referred to OHSU, or like institutions, for a “Dutch Protocol” of puberty blockers and cross-sex hormones. Further, the nurses should expect such referrals to comprise 3 percent of the children in their care.
OHSU has since taken down the URL, but you can find the original PDF from which all quotes are taken here.
What was perhaps most astonishing about this reply went without comment by the nurses or their employer: The citation upon which the 3 percent prediction was based didn’t remotely say what it was derived from. Why didn’t anyone notice or object? To understand that, one must understand the evolving relationship between the gender industry and Oregon regulators.
Oregon’s Policies Are Hardly Rooted in ‘Good Faith’
OHSU is Oregon’s premiere high-volume gender center, with more than a century of experience performing gender-based medical intervention on adults. Lawmakers increasingly trust OHSU to help reshape policies “at the system, community, state and federal level,” and to shape education from kindergarten to doctoral studies, so that on-demand gender-based medical intervention, subsidized by state Medicare, is available to all ages.
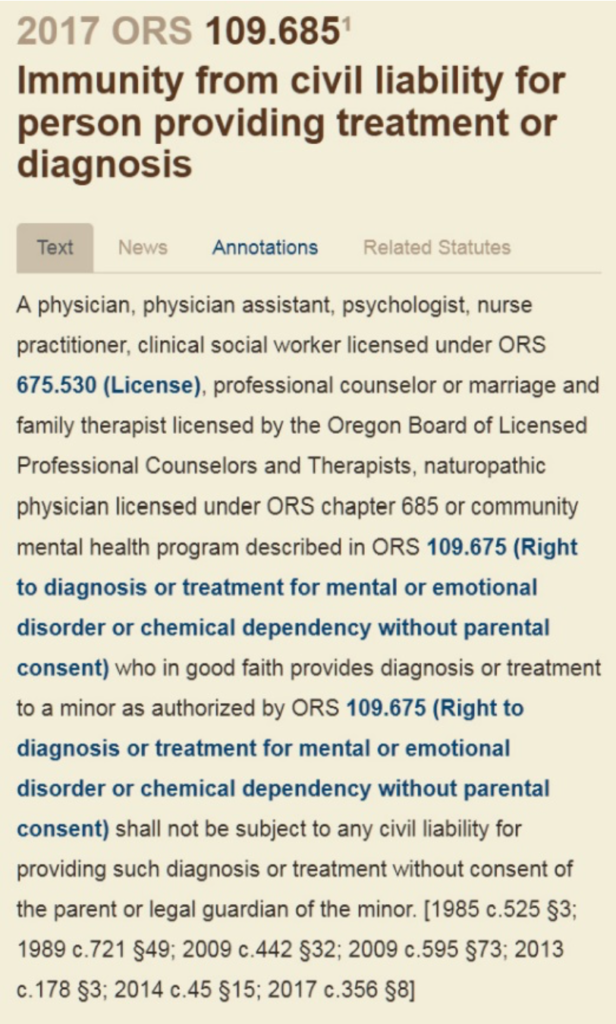
The effect on Oregon’s regulatory atmosphere is palpable. Oregon law now considers anyone over 15 an adult for the purpose of consenting to medical gender intervention without parental knowledge (14 when the intervention happens in a mental health setting); and health providers are immune from liability for acting against parents’ objections “in good faith.”
But is “good faith” the proper terminology to describe a public policy set by those who stand to gain financially from it? Economist George Stigler gave it a different name: regulatory capture. Stigler noted that regulatory policies undertaken on the advice of the industry they regulate tend to become indistinguishable from the industry’s marketing objectives.
Stigler would probably not be surprised to learn that, having relied on the good faith of the gender medicine industry, Oregon now:
- Allows adverse gender surgery outcomes to go largely untracked
- Restricts health workers’ right to advise patients about the risks of gender-based medical intervention
- Strips custody from parents who object to gender-based medical intervention on their children.
Nor would Stigler be surprised that no one in the psych ward balked at the idea that 3 percent of children should be referred for gender intervention.
OHSU Distorts the Figures
To put the 3 percent claim in context, it’s helpful to consult numbers the American Psychological Association (APA) published just a few years earlier. In its “Diagnostic and Statistical Manual, Fifth Edition” (DSM-5), the APA estimated that patients believing themselves to be in the wrong body were exceedingly rare, historically comprising only 0.005-0.014 percent of the male population, and 0.002-0.003 percent of the female population.
By contrast, the OHSU told the Oregon nurses they should refer children for gender intervention at a rate between 200 and 1,500 times the DSM-5’s figures (0.03 ÷ 0.00014 = 214.29 for the lower limit of the range, to 0.03 ÷ 0.00002 = 1500.00 for the higher limit).
Further, as mentioned, the Portland Public School survey offered in support of that claim concluded no such thing. It didn’t even survey children. Its full title (foreshortened in the training’s citation), included the tagline “A School Climate Survey for Parents and Guardians.”
Only twice did it mention gender, neither time referencing children, and not a single parent responded to those questions in the affirmative:
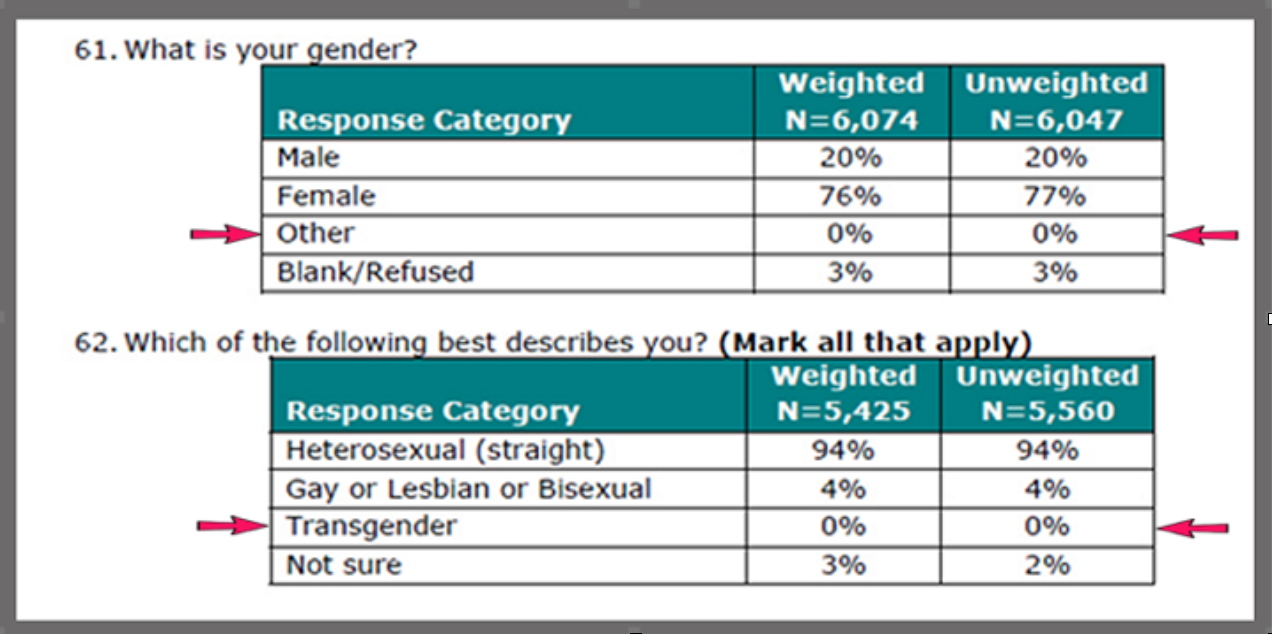
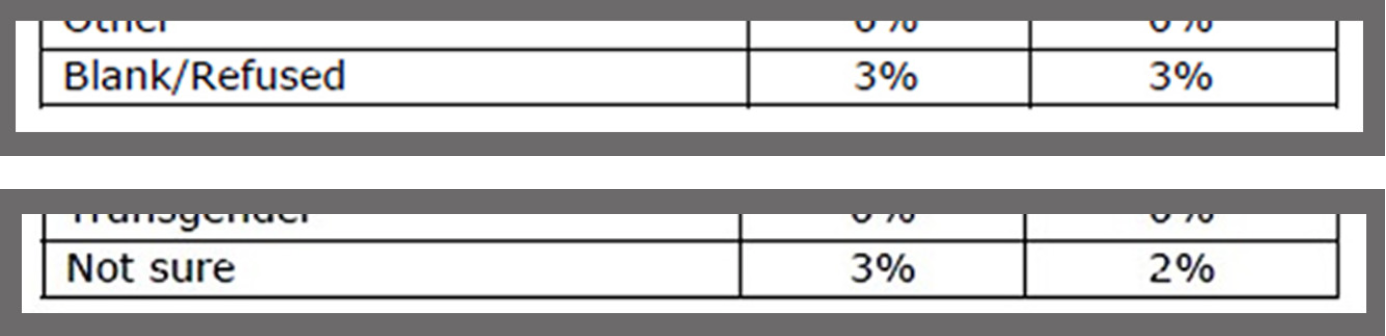
The only 3 percent value in the survey referenced the number of parents who were confused by the question or who refused to answer:
Yet in a hospital training, administered by people with advanced degrees to other people with advanced degrees, no one questioned the assertion that 3 percent of local kids were in the wrong body and that the hospital on the hill could give them the right one.
‘A Quality Improvement Project’
The cultural trajectory — from “first do no harm” to “no holds barred” — that Oregon is traversing under a regulatory framework shaped by gender service providers, is reflected in the disparate responses the two institutions gave when asked about the invalid 3 percent citation.
The suburban hospital took pains to distance itself from the matter: “OHSU did not ‘teach’ Willamette Falls staff. … This was not a research project or any kind of formal collaboration between Providence and OHSU,” said Jean Marks, Providence Health and Services media contact.
But OHSU’s representative made no such disclaimer. It was OHSU’s digital commons that published the account in a spring 2017 paper entitled “Increasing Transgender Cultural Competency with Youth Through an Online Training Module: A Quality Improvement Project.”
The document described a six-month “transgender cultural competency … training module,” which an OHSU graduate student administered to nurses from the Child and Adolescent Psychiatric Unit (CAPU) of Willamette Falls — a branch of Oregon’s largest private employer, Providence Health System — with supervision by the CAPU’s nurse manager and a green light from the institutional review boards of both hospitals.
Training Pediatric Nurses in Gender Affirmation Theory
Because OHSU has denied nothing in the document, and its author clearly believed the training took place as described, I’ll refer to the event here as the “CAPU training” per its own description, with disclosure that Willamette Falls disputes that description.
According to the description of the training, nurse volunteers from the CAPU learned gender affirmation theory, a treatment protocol in which children’s identity struggles are taken as evidence that they are in the wrong body and will commit suicide unless medical professionals give them a new one. This model rejects traditional “gatekeeping,” such as waiting periods and psychiatric evaluation, and proceeds directly to pharmacological and surgical intervention on demand.
The affirmation model was controversial at the time of the CAPU training and has only become more so in the intervening years, with government ethics inquiries pending in the United Kingdom, Sweden, and Australia, even as states such as Oregon have enshrined affirmation theory’s teachings into law.
Chief among the objections to the affirmation model is that it disproportionately targets for sterilization children who are mentally fragile or disabled.
How On Earth Did This Become Oregon’s Policy?
Stigler believed regulatory capture was a top-down process, with industry forcing its will upon regulators and the public. But this gives short shrift to citizens’ agency. For example, the CAPU training module was entirely voluntary, at the request of an audience that by all accounts willingly suspended its disbelief about the numbers cited regarding Portland school kids.

Like the subjects of Hans Christian Andersen’s naked emperor, Oregonians have silently acquiesced to the invisible-cloth logic their homegrown industry has proffered. We can perceive that also in OHSU’s response, when it was asked to explain the discrepancy between the CAPU training’s claim of 3 percent and its supporting citation:
The data regarding prevalence of transgender youth is sparse because demographic information related to both sex assigned at birth [sic] and gender identity of young people isn’t routinely captured, and when captured, it is inconsistent and not meaningfully used and shared. The only reference to prevalence of trans youth (only 13-17 years old) that I am aware of and willing to cite is a 2017 report titled ‘Age of individuals who identify as transgender in the United States,’ and that report is likely an underestimation.
—Amy Penkin, MSW, LCSW, OHSU Transgender Health Supervisor
This explanation cites a 2017 report that arrived at numbers an order of magnitude smaller than the errant 3 percent figure, but OHSU attributes the discrepancy to data scarcity.
Data scarcity is indeed a problem with gender-affirmation theory, leading many countries to rethink their regulatory trust in gender industry claims. As the British Medical Journal elucidated after a top U.K. gender health official resigned:
There are significant problems with how the evidence for Gender-affirm[ation] … has been collected and analysed that prevents definitive conclusions to be drawn. … [T]he evidence is limited by small sample sizes; retrospective methods, and loss of considerable numbers of patients in the follow-up period. The majority of studies also lack a control group.
The U.K.’s qualms were prompted by the discovery that, after a decade of reliance upon the gender industry to set policy, the number of girls intervened upon increased more than 4,000 percent, with many suffering from comorbid mental health and developmental issues. It remains unclear whether the United States will heed European warnings about regulatory capture or follow Oregon’s incautiously silent steps.
The U.S. Needs to Ask the Questions Oregon Didn’t
The CAPU training incident is precautionary: The same OHSU spokeswoman who explained the faulty 3 percent citation by appealing to data scarcity had only months before signed a consensus statement telling a federal court that gender-affirmation policies were based upon “a substantial body of research.”
Oregon did not ask, as the United States still might: To what extent does the CAPU training’s errant citation reflect upon the quality of the “substantial body of research” behind that “consensus” about gender medicine? And to what extent might public health policies based on this “consensus” be helping to turn the erroneous 3 percent figure into reality?
Although the suburban hospital’s repudiation of the CAPU training suggests Oregonians regret their silence, their die is cast: Within weeks of Oregon’s decision to offer Medicare funding for gender services, OHSU gained a backlog of “more than 100 transgender children.” The United States now stands at a crossroads Oregon has left behind.
Intervene Before This Becomes a Self-Fulfilling Prophecy
On one hand, Medicare regulators are duly skeptical about gender industry data:

And the U.S. Senate has shelved the Equality Act, which would expand the transgender medical industry nationwide, after the House failed to take measures addressing the civil rights repercussions caused by similar legislation in states such as Oregon. On the other hand, the U.S. gender industry continues to conflate “consensus” with evidence and to censure scientists who question that evidence.
And the Centers for Disease Control and Prevention now asserts that 1.8 percent of surveyed children — many of whom happen to live near major gender centers — believe themselves to be in the wrong bodies. The question remains: Will Americans check the citations and speak up? Or will they stand silently by as these numbers too become a self-fulfilling prophecy?












{kind=link}